Telangana TSBIE TS Inter 2nd Year Economics Study Material 2nd Lesson Demography and Human Resource Development Textbook Questions and Answers.
TS Inter 2nd Year Economics Study Material 2nd Lesson Demography and Human Resource Development
Essay Questions
Question 1.
Explain the theory of demographic transition.
Answer:
Theory of Demographic Transition :
The theory of demographic transition was propunded by W.S. Thomson and F.W Notestein. They explain the theory in three stages. This theory explains the effects of changes in birth rate and death rate on the growth rate of population.
According to the ‘theory of demographic transition’, every country passes through three stages in which birth and death rates are typically associated with economic development. First Stage: Jn the first stage, the country is backward and both birth and death rates are high. High birth rate is matched by ap equally high death rate, and thus, the population remains more or less stable. Death rate are high in the first stage of agrarian economy on account of poor dites, primitive sanitation, absence of effective medicl aid, low level of standard of living, poor housing conditions, absence of opportunities for education and unscientific and irrational outlook.
Birth rates are also high in this stage due to lack of education, superstitions, social beliefs and customs about the size of family and early manages. In this stage, the actual growth rate of population (birth rate – death rate) is not high, because, high birth rate is balanced by high death rate. This stage prevailed in India before 1921.
Second stage :
This stage is characterised by rapid growth of population due to substantial reduction in the mortality rate and no corresponding decline in the birth rate. With the beginning of the process of development, the living standards improve, the education expands, medical and health facilities increase and the state makes special efforts to check the contagious diseases. Rise in income levels enable the people to improve diet. All these factors bring down the death rate.
But due to agrarian society with no mass education, attitude of the people towards the size of family does not change radically. So, the birth rate remains high. Thus, high birth rate and rapidly falling death rate contribute to high growth rate of population. In this stage, population increases at an alarming rate and economists call it as population explosion. India and faced this situation during the period 1951 – 1991.
Third stage :
Economic development rapidly changes the character of the economy from an agrarian to Industrialized one. Industrialisatioln compels people to change their attitudes towards the size of family and they recognise the merits of samll family. Education helps the people in right way of thinking. For working women, upbringing of children is not an easy task. People want to maintain reasonable standard of living. All these reinforce people’s desire to have smaller families. So, birtha rate declines significantly. The characteristics of the third stage ae low birth rate, low death rate, small family and low growth rate of population.
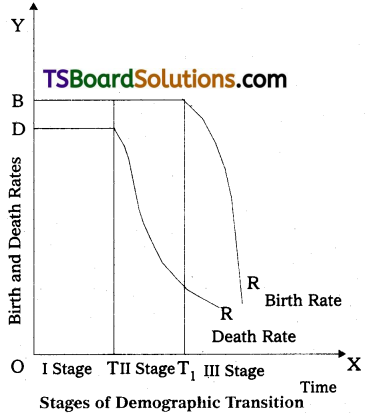
In the above figure the time for different staages is taken on the horizontal axis and annual birth and death rates per 1,000 population on the vertical axis. In the first stage, 0 to T, birth and death rates are high and growth rate of population is very much low. But, in the second stage, T to Tj, though the death rate is falling, birth rate is remaining high and this leads to higher growth rate of population and its result is population explosion. However, in the third stage, after Tp both birth and death rates are falling and again growth rate of population will be low and population increases at a slow pace.
![]()
Question 2.
Examine the trends of population growth in India. ,
Answer:
India possesses 2.4% of the total land area of the world, and with its population of 1.3 billions in 2017 it has a share of 17.6% in the world population. India is the second largest country in terms of population size after China. India accounts for only 7.3% of world GDP in 2017. These facts indicate that the pressure of population on the land in India is very high.
According to 1901 Census, India’s population was 236 million and according to 2011 Census, the popoulation was 1210 million and it was 1.3 billions in 2017. In a period of 116 years, the population of the country has increased by 1064 million.and growth trends of India’s populatin during 1891 – 2011.
a) During the first phase of 30 years (1891 to 1921), India’s population grew from 236 million in 1891 to 251 mollion in 1921 i.e., just by 15 million. The compound annual growth rate was 0.19% per annum for the period. Birth and death rates were more or less equal during this period.
b) During the second phase from 1921 to 1951, India’s population grew from 251 million in 1921 to 361 million in 1951 i.e., by 110 million. The compound annual growth rate of population was 1.22% which was considered as moderate. The main reason for this was a decline in death rate from 49 per thousand population to 27 per thousand population and a very small decrease in birth rate from 49 per thousand population to 27 per thousand population and a very small decrease in birth rate from 49 per thousand population to 40 per thousand population. India had entered into the second phase of demographic transition during this period with a steady but low growth rate of population. The year 1921 is regarded as great dividing year of population because of decrease in population and a turning point for the increase in the growth rate of population.
c) During the third phase from 1951 to 1981, the population of India grew from 361 million in 1951 to 683 million in 1981. There was a record growth of population by 322 million in this.30 years. The compound annual growth rate of 2.14% is nearly double the growth rate of the previous phase. Due to the planning, many measures of death control were undertaken. This resulted in a further and sharp decline of death rate to a level of 15, but the birth rate fell very slowly from 40 to 37 during this period. So, there was a population explosion during this pahse.
d) During 1981 to 2011, India’s total populatio increaed from 683 million to 1210 million indicating an increase of 77% during the 30 year period. The annual average rate of growth of population during this period was 1.84%.
1. Birth Death and Infant Mortality Rates :
The growth of populatin was .checked by the high birth and high death rates in India before 1921. Birth rate during 1901-1921 fluctuated vetween 46 and 49 per thousand papulation and the death rate between 44 and 49. So, the growth of population was little or negligible. After 1921, a clear fall in death rate is noticeable. Death rate which was at 48.6 per thousand in 1911- 20 came down to 7.1 per thousand in 2010-11.
But, the birth rate showed a slight decline initially and due to family planning drive birth rate also declined to 21.8 per thosand in 2010 – 11. There is a steady fall in the infant mortality. In the second decade of the 20th century, infant mortality rate was 218 per 1,000 live births and it is 47 per 1,000 live births in 2010. Over the years, maternal mortality has also declined. Itwas 210 per 1 lakh live births in 2007 – 2009.
2. The sex Ratio :
The sex ratio is defined as the number of females per 1.000 males. The sex ratio declined from 972 in 1901 to 946 in 1951 and to 927 in 1991. It is a disturbing feature. Subsequently there is a marginal improvement in the sex ratio. It is increased to 933 in 2001 and to 940 in 2011. Kerala alone shows a higher proportion of females of 1,084 per 1,000 males in 2011. In Punjab and Haryana, females account for 893,and 877 per 1,000 males in 2011 respectively which are at the bottom. Poverty, higher female infant mortality rates, high mortality rates among women in reproductive ages and sociological factors including a bias against female births are responsible for declining sex ratio.
3. Age Composition :
The study of age composition is useful in determining the proportion of labour force in the total population. The working age of the population is considered as 15 – 60 years, the proportion of child population in the 0 – 14 years age group is 35.6% in 2001 and this is lower than the earlier figures. The working age pertains to 15 – J60 yearws is called as productive age group. Both the child population and old population are dependent of the productive age group.
Both the child population and old population are dependent on the productive age group for their maintenance and sustenance, there is a decline in the dependency load of the population and increase in the share of the productive age group. Demographic dividend is likely to manifest in the gradual increase in the working age group of 15 – 60 years. A recent report from the UN population Fund estimages that India’s working age population will reach 65% by 2030. India will also enjoy the longest demographic dividend compared to any other country till 2055.
Question 3.
What are the causes for rapid growth of population in India?
Answer:
In India, the population has increased rapidly due to a steady decline in the death rate while birth rate remained high and this led to population explosion. Examination of causes for decline in the death rate and high birth rate is necessary.
Causes of Population Explosion :
Mainly there are three causes for a rapid growth of populatioon of a country: i) a high birth rate, ii) a relatively lower death rate and iii) immigraion. Immigration does not have much impact on India’s population growth.
I. Causes of Decline in the Death Rate :
1. Elimination of Famines :
Recurrence of famines in India under the British rule was a major cause of high mortality rate. Since independence, the situation has considerably improved as the famines have not occured on a large scale and the problems due to droughts have been met.
2. Control of Epidemics :
Cholera, small pox and malaria were the major causes of epidemics before independence. Now, small pox is eradicated completely and cholera and malaria are very much under control. There has been some decline in the incidence of tuberculosis, but, still it is a major killer in India.
3. Other Factors :
Factors such as supply of drinking water, sanitation and hygiene, spread of education, expanded medical facilities, immunisation, poverty eradication programs and improvement in living standards will reduce mortality rate.
II. Causes of High Birth Rate :
The birth rate is high in India. Except in the states of Kerala, Tamil Nadu and Goa, birth rate has not declined significantly in India due to a number of economic and social factors.
A. Economic Factors : Three economic factors namely :
1. Predominance of Agriculture :
In agrarian societies, children have never been considered as an economic burden. The peaks of productive activity in agriculture require more labour. Hence, in a predominantly agricultural economy of India, bigger families exist.
2. Urbanisation :
Due to staggering industrialisation, the process of urbanisation is slow in India and it failed to generate social forces which reduce, the birth rate.
3. Poverty :
Poverty in under developed countries results in high fertility. At a lower income level of the family, the benefits of having an additional child to the family generally exceed the cost of his upbringing. The poor have no other economic asset than their own labour. Hence, they assume that mote the number of earners in the family, the moe family earnings. The lower survival rate also reinforces the preference for children. Thus, poverty is a major factor which works against the acceptability of family planning programme by the poorer sections.
B. Social Factors :
Universality of marriage, lower age at the time of marriage, religious and social superstitions, joint family system, lack of education and a very limited use of contraceptives are some of the social factors which limit the decline in fertility.
1. Universality of Marriage :
Marriage is both a religious and a social necessity. With the spread of education, attitude of people towards marriage will change and some may decide not to marry. But, in a slow moving society where education is also not spreading fast, the above situation can not be expected.
2. Lower Age at the Time of Marriage :
The relatively lower age at the time of marriage is responsible for high fertility. Mean age at marriage for females is 18.3 years and for males 22.6 years in 2001 in India. Due to this, fertility is bound to remain high.
3. Religious and Social Supersititions :
Due to religious and social superstitions, many people prefer to have children irrespective of their economic position. Children are regarded as God given and preordained.
4. Joint Family System :
The joint family system induces young couples to have children, though they are unable to support them. Because, their economic burden is borne by the earning members. However, the process of disintegration of joint family system has not only started, and it reached to its peak level.
5. Lack of Education :
According to 2011 Census, 74% of the population is literate in India. The percentage of literacy among women is much lower i.e., 65.5% as compared to 82.1% among men. Education alone can change the attitude of the people towards family, marriage and birth of a child. Illiterate people cannot be exposed to rational ideas. There is an inverse relationship between education and fertility.
6. Use of Contraceptives :
Though the government is carrying the idea of family planning and contraceptives are made available, the response is not encouraging from certain sections due to lack of education and religious dogmas. With the expansion of education, people will certainly develop a preference for a smaller family.
![]()
Question 4.
What are the measures required to control population explosion?
Answer:
Remedies for population Explosion :
Three fold measures are required to deal with the population explosion. These are as followed. .
I. Economic Measures
1. Expansion of the Industrial Sector :
Industrial workers are aware of the difficulties in getting employment and are interested in restricting the size of their family. They realise that in order to raise their standard of living they must restrict the size of their family. Hence, rapid industrialization is required.
2. Creation of Employment :
Urbanisation and industrialisation are mutually interdependent. We have to create more job opportunities in cities and villages and this may be a powerful check on the growth of population. The housing problem and the cost of upbringing of children in urban areas usually prohibit people from having big families.
3. Equitable Distribution of Income and Removal of Poverty :
Once the poor people start getting basic amenities of life, they have no economic compulsion to have more children and their attitude towards the size of family will undergo a change. For this, equitale distribution of income and right to work with living wage are necessary.
II. Social Measures :
Population explosion is not only an economic problem but also a social problem. Many causes of population explosion are deep rooted in the social life. Social evils must be curtailed to bring down the birth rate.
1. Education :
Most educated people delay their marriage and prefer samll family. Education, by making a frontal attack on orthodoxy and superstitions, induces people to practise family planning. When boys and girls go to schools and colleges, marriages will be delayed and this reduces the reproductive span of women. The link between female literacy and fertility is clear. But the 2011 Census has shown that the female literacy rate is 65.5% as against the male leteracy rate of 82.1%.
2. Status of Women :
The position of women is inferior to that of men both socially and economically. That is why, educatilon is less among women and hence, they are quite indifferent to family planning. People will not shed wrong notions such as preference for male child, unless the status of women improves. In a backward society, women have no choice regarding her children.
3. Age of Marriage :
Fertility depends on the age of women at marriage. In India, average age at marriage is low. Under the Child Marriage Restraint Act, 1903, the minimum age of marriage was 18 years for men and 15 years for women. In 1978, this act was amended to raise the minimum age to 21 years for men and 18 years for women. But, an effecive implementation of legal enactments is impossible due to fears in rural areas about the safety of unmarried girls, illiteracy, lack of knowledge about laws and inadequate registration system.
III. Family Planning Programme
Importance of the family planning programme as a device to control population explosion is now universally recognised. Widespread use of contraceptives has contributed most to China’s success. About 85% of married women of child-bearing age use contraceptives in China a against 41% in India. The following aspects have to be discussed in this respect.
1. Public Information Programme :
For raising the level of consciousness, couples in the reproductive age are to be informed about the usefulness of family planning. The government is using all media to publicise the importance of family planning. Once they catch the idea of family planning, they themselves starty practising it.
2. Incentives and Disincentives :
The government has introduced different schemes in which incentives are given to those who accept family planning. Cash prizes have given some inducement to the people to go for sterilisation. In India family planning is voluntary. During the emergency, some excesses were committed and forcible sterilisations were done. In fact, atleast for some time, compulsory family planning is required.
3. Family Planning Centres :
Establishment of family planning centres is an integral part of family planning programme. These centers provide various clinical facilities needed for family planning. Contraceptive distribution centres are also playing very important role.
4. Research :
Research in the field of demography, communication action, reproductive biology and fertility control must be given priority. The government of India has realised this to obtain maximum results.
Question 5.
Describe the occupational distribution of populatin in India.
Answer:
Occupational and Sectoral Distribution of Population in India:
The occupational structure of a country refers to the distribution of its population according to different occupations. Occupations are divided into three types :
i) Agriculture, animal husbandry, forestry, fishery, etc. are collectively known as primary activities. They are primary as their products are essential for human existence and these are carried on with the help of nature,
ii) Manufacturing industries, both small and large scale,- are known as secondary activities,
iii) Transport, communications, banking and finance services are tertiary activities and these help the primary and secondary activities.
Economic Development and Occupational Distribution :
Transfer of population from agriculture to industry and eventually to services is considered as an index of economic development. Colin Clark argues that “a high average level of real income per head is always associated with a high proportion of the working population engaged in tertiary industries, low real income per head is always associated with a low proportion of the working population engaged in tertiary production and a high percentage in primary production”. According to Hans Singer, economic development will be achieved by transforming a 85% agricultural dependent country in to just 15% agriculturally dependent country.
Occupational Distribution of Working Population in India :
Over the period 1951 to 2010, agriculture remained the main occupation of the people, Over the period 1951 to 1971, the percentage of labour force engaged in primary sector remained unchanged at around 72%. There is a major change in the period 1991 – 2010 with the percentaghe of labour force in the primary sector falling to 51% in 2010 from 67% in 1991.
After independence, the process of industrialisation was accelerated and the absolute number of persons getting employment in the secondary sector substantially increased. Since the population growth is rapid, and the rate of industrial growth fell short of expectations, transfer of labour force from primary sector to secondary sector and to services sector did not take place. In 2010. 22% of the working population is employed in the secondary as against 11% in 1951. During the period 1991 – 2010 the proportion of labour force in the secondary sector increased significantly from 13% to 22%.
The proportion of workers employed in the tertiary sector increased over the 60 years from 1951 to 2010.27% of the working population is employed in teh tertiary sector aas against 17% im 1951.
It is clear that over the first four decades of planning (1951 – 1991), the occupational structure of Indiain population almost remained unchanged. Only in the later two decades (1991 – 2010) some important changes are visible. In India, due to rapid growth of population, traditional agriculture with low labour productivity and slow pace of industrialisation, occupational structure has not undergone significant changes.
![]()
Question 6.
Explain the new population policy, 2000.
Answer:
National Population Policy, 2000 :
The National Population Policy, 2000 outlined immediate medium and along term objectives. The immediate objective is to meet needs of contraception health infrastructure, health personnel and to provide integraged services for basic reproductive and child health care. The medium term objective is to reduce the total fertility rates to the replacement level by 2010. The long term objectives is to stabilise the population by 2046. A.D.
- Reduction of infant mortality rate below 30 per 1,000 liver births.
- Reduction of maternal mortality rate below 100 per 1,00,000 live births.
- Universal immunisation.
- Achieve 80% deliveries in regular dispensaries, hospitals and medical institutions with trained staff.
- Access to information, contgain AIDS, prevention and control of communicable diseases.
- Incentive to adopt two child small family norm.
- Facilities for safe abortions to be increased.
- Strict enforcement of Child Marriage Restraint Act and! Pre – Natal Diagnostic Tech-niques Act.
- Raising the age of marriage of girls not earlier than 18, and preferably raising it to 20 years (or) more.
- A special regard for women who marry after 21 and opt for a terminal method of contraception after the 3 second child.
- Health insurance cover for those below the poverty line who undergo sterilization after having t®w children.
- Achieve universal access to inforamtion, counselling and services for fertility regularisation and contraception.
- Bring about convergence in implementation of relat3d social sector programmes to make family welfare a people centred programme.
The National Commission on population has been set up to review the implementation of the National Population Policy from time – to – time. State level commission on population also have been setup with the objective of ensuring the implementation of national population policy.
Question 7.
Examine the role of education in eonomic development.
Answer:
Role of Education in Economic Development: Education and skill training are important for human resource development.
1) Education and economic development :
Investment in education promotes economic development. According to Todaro and Smith, education helps to increase knowledge and skill and so that more productive labour force can be created. Employment and income earning opportunities will increase due to education. Educated leaders can be created. Education provides skill and encourages modern attitudes.
2) Reduction of income inequalities :
Universal education will improve the human ca-pabilities of the people and helps them in increasing their earnings.
3) Rural development :
Education provides knowledge to the rural people and they can overcome ingnorance and superstitions. If the farmers are educated they will adopt new agricultural techniques. Education provides skill to the people to set up cottage industries and this reduces disguised enemployment.
4) Family planning :
Education enlightens people of the need to improve their standards of living and so to restrict the size of their families. Education serves as the best method of family planning in the long run aned it is also proved. If more women are educated and seek employment, fertility ratges will decline as upbringing to children becomes difficult for women employees.
5) On – the Job Training :
Many firms provide on-the-job training to their workers, because improvement in human capital increases the roductivity of physical capital. On – the – job training increases the skill and efficiency of workers and so increases in productivity and production.
Spill over income gains to the present and future generation, the meeting of skilled man-power requirements, research in science, promotion of responsible behivious, political stability, transmission of cultural heritage etc., are also possible in the society due to increased education.
If people don’t get suitable education, they not only forego much mofe at present but also in the future.
Question 8.
Describe the health policies and programmes adopted in India.
Answer:
Health Policies in India :
On the basis of recommendations by the Health Survey and Development Committee (More Committee, 1946) and the Health Survey and Planning Committee (Mudaliar Committee, 1961), the government of India prepared ing the health standard.
Objectives of this programme :
- Provision for the control of epidemics
- Providing health services; and
- Training of employees in the health department and the development of primary health centres in rural sector.
During the 9th and 10th Five yedr plans, efforts were intensified to improve the health status of population by optimising coverage and quality of care. Eleventh Five year plan proposed a comprehensive approach that covers individual health care, public health, sanitation, clean drinking water, access to food and knowledge of hygienes and feeding practices. The plan set the following targets to be achieved by the end of plan period (2011 -12).
- Reducing maternal mortality rate to 100 per 1 lakh live births.
- Reducing infant mortality rate to 28 per 1,000 live births.
- Reducing total fertility rate to 2.1.
- Providing clean drinking water to all by 2009.
- Reducing malnutrition among children of age group of 0 – 3 years by 50 percent.
- Reducing anemia among women and girls by 50%.
- Raising sex ratio for age group of 0 – 6 years to 935 per 1,000 by 201 -12 and 950 by 2016-17.
In India, life expectancy at birth was 41.2 years for the dedcade 1951-61 and improved to 68.5 years as per census 2011. Infant mortality rate is 47 per 1,000 live births in 2010 as against 146 per 1,000 in 1951. During 2001 – 03 maternal mortality rate was 301 per 1 lakh live births and it was reduced to 200 by 2010. Improving birth attendance and midwifery facilities at a rapid rate are required to reduce maternal mortality rate in India. Total fertility rate (total number of live births by a woman during her entire reproductive period) in the early 1950s was 6.0 and it has come down to 2.4 in 2011.
Health Programmes in India :
The 11th Five year plan aimed for inclusive growth by introducing National Rural Health Mission and National Urban Health Mission.
i) National Rural Health Mission (NR HM) :
This intends to increase access and utilizztion of quality health by strengthening healht infrastructure. It was planned to have (i) 5 lakh Accredited Social Health Activists (ASHAs) by 2008, (ii) All sub – centres functional with 2 Auxiliary Nurse Midwives (ANMs) by 2010. (iii) All Primary Health Centres (PHCs) to be provided 3 staff nurses for 24 hours on all days by 2010. (iv) 6,500 Community Health Centres to be establisghed, strengthened with 7 specialists and 9 staff nurses by 20121 (v) 1,800 Taluka Hospitals and 600 District Hospitals to be strengthened by 2012. (vi) Mobile Medical Units for each district by 2009.
ii) Janani Suraksha Yojana (JSY) :
This scheme has the dual objectives of reducing maternal and infant mortality by promoting institutional deliveries. It is 100% centrally sponsored, and integrates cash assistance with medical care. A gradual approach of increasing istitutional capacity and encouraging institutional deliveries will ensure success of the scheme. Under NRHM, out of 184.25 lakh institutional deliveries in the country (as on 1st April, 2007), JSY beneficiaries Were 28.74 lakhs.
iii) National Urban Health Mission (NUHM) :
This programme covers all cities with a population of 1 lakh and above.
In relation to health, the 2018-19 Union Budget announced a flagship National Health Protection Scheme to cover over 10 crore poor and vulnerable families, approximately 50 crore beneficiaries, providing coverae upto Rs. 5 lakh per family per year for secondary and tertiary care hospitalization. This will be the World’s largest government funded health care programme. The revised estimate for the National Health Insurance Programme Rashtriya Swasthya Bima Yojna (RSBY) for Financial year 2018 -19 was Rs. 2,700 crore, and the allocation in the Union Budget for Financial year 2019 – 20 is Rs. 6,556 crore.
iv) Clean Drinking Water and Sanitation :
Unsafe drinking water increases the risk of diseases and malnutrition and water – borne diseases which effect health adversely. That is why, clean drinking water is a vital necessity. Lack of sanitation is directly responsible for several water borhne diseases.
According to World Development Indicators (2008), access to improved water source was available to 86% of the population in 2004. According to World Bank, 33% of the population in India had access to improved sanitation facilities in 2004.
A big initiative of the NDA government has been the Swachh Bharat Mission (SBM) launched on October 2, 2014 with the goal of making India Open Defecation Free (ODF) by October 2019. The main aim of SBM has been the construction of toilets. Official statistics by the Ministry of Drinking Water and Sanitation claim that as of January 2019, 92.2 million toilets had been built since the inception of SBM, leading to a 98 percent rural sanitation coverage with 604 districts and 5,52,000 villages declared ODF.
![]()
Question 9.
What are the different indices to measure human development? Explain them.
Answer:
The United Nations Development Programme (UNDP) introdeuced the HDI in its first Human Development Report, 1990, under the guidance of Mahbub – UI – Haq, an economist from Pakistan.
UNDP Human Development Report, 1997 descruves human development as “the process of widening people’s choices and the level of well – being they achieve. Regardless of the level of development, the three essential choices are to lead a long and healthy life, to acquire knowledge and to have access to the resources needed for a decent standard of living.
According to Mahbub – U1 – Haq, “the difference between the economic growth and the human development schools is that the first exclusively focuses on the expansion of only one choice income – while the second embraces the enlargement of all human choicex – whether economic, social, cultural of political”.
HDI measures the average achievement in three basic dimensions of human development and these are : (i) a long and healthy life as measured by life expectancy at birth, (ii) knowledge as measured by the adult literacy rate and the gross enrolment ratio and (iii) a decent standard of living as measured by GDP per capita (PPP US$).
Before calculating HDI, an index for each of the three dimensions is creatd. For this, maximum and minimum values are chosen for each indicator as given below.
Performance in each dimension is expressed as a value between 0 and 1 by applying the formula given below :

The HDI is calculated as a simple average of the dimension indices.
According to HDR 2011, countries are grouped under four categories :
(1) countries in the HDI range 0.8 and above are in the very high human development group, (2) countries in HDI range 0.7 to 0.8 are in the high human development group, (3) countries in the HDI range 0. 5 to 0.7 are in the range of medium human development group, and (4) countries in the HDI range less than 0.5 are in the low human development group.
India which was ranked at the 134th position in HDI in 1975 had improved its rank to 128 in 2005, but in 2011 its position slipped again to 134th rank. Norway ranked first and Australia ranked second in 2011.
India was at 135th position in HDI out of 187 countries in 2013. As per annual HDI – 2019. report, India ranked at the 129th position in 2018 out of 189 countries.
Human Development Report, 1995 introduced two global gender indices. These are : (1) Gender related Development Index (GDI) and (2) Gender Empowerment Measure (GEM).
The GDI attempted to capture achievements through the same set of basic capabilities as included in the HDI – life expectancy, educational attainment and income. HDI will be adjusted for gender inequality.
The Gender Empowerment Measure (GEM) indicates whether women are able to participate actively in economic and political life. It focuses on political participation (women’s share in parliament seats), economic participation (share in higher level and professional positions) and power over economic resources (income gaps).
2) Human Poverty Index (HPI) :
Human Development Report, 1997 introduced the concept of Human Poverty Index. This index concentrates on deprivation in three essential elements of human life already reflected in HDI – longevity, knowledge and a decent living standard. HDR, 2009 used the following variables for calculating HPI : (i) percentage of people expected to die before age of 40 years, (ii) percentage of adult illiterates, (iii) percentage of people with access to health services and to safe drinking water and (iv) percentage of malnourished children under five years.
3) Gross National Happiness Index :
Countries like Bhutan are measuring their development with gross national happiness index. There is a need to bring a change in the existing method of measuring the development.
Gross National Happiness has been devised by Bhutan as an alternative indicator for GDP to measure progress or development. The term Gross National Happiness (GNH) was coined by the Fourth king of Bhuta, Jigme Singye Wangchuck in the 1970’s, The concept implies that sustainable development should take a hollistic approach towards notions of progress and give equal importance to non – economic aspects of wellbeing. The GNH index is constructed based upon a multidimensional methodology known as the Alkire – Foster method.
The concept of GNH is explained by four pillars :
good governance, sustainable socio-economic development, cultural preservation and environmental conservation. These four pillars are further classified into nine domains : Psychological wellbeing, health, educatin, time use, cultural diversity and resilience, good governance, community vitality, ecological diversity and resilience, and living standards. All domains are weighted equally.
Question 10.
Explain the views of Amartya Sen on Human Development.
Answer:
Views of Amartya Sen on Human Development :
Amartya Sen is the first Indian who won the Nobel Prize of Economics. Amartya Sen’s book “Development as Freedom” was published in 1999. He argues that the development is the process of expanding human freedoms that people enjoy.
Sen says that freedom is both the primary end and the principal mean of development. For this, he gives two reasons :
(i) the only acceptable evaluation of human progress is enhancement of freedom and (2) the achievement of development is dependent on the free agency of people. Growth of GNP or of Individual incomes can be very important as means to expanding the freedom enjouyed by the people, Freedom depends on other determinants also, such as social and economic arrangements (facilities for education and health care) and political and civil ritghts (the liberty to participate in public discussion and scrutiny). Industrialization or technololgical progress or social modernization can substantially contribute to expanding human freedom, but freedom depends or other influences also.
Freedom creates growth. Freedom is a principal determinant of individual initiative and social effectiveness. It enhances the ability of individuals to help themselves. Raising human capability improves the choices, well – being and freedom of people and also their role in influencing social change and economic production, /economic security derives from freedom. The institutional arrangements are also influenced by the freedoms, though the liberty to participate in social choice and in the making of public decisions.
He mentions five freedoms :
political freedom, economic facilities, social opportunities, transparency guarantees and protective security. Political freedoms (free speech and elections) help to promote economic security. Political freedom and civil rights have to be achieved as a direct good in their own right, but not thorugh the achieving GDP growth. Economic facilities (opportunities for participation in trade and production) will help to generate personal abundance and public resources for social facilities. Social opportunities (education and health) facilitate economic participation. Freedom of different kinds can strengthen one another.
Sen advocates government measures to support these freedoms by providing public education, health care, social safety nets, good macro economic policies, productivity and environment protection.
Development requires the removal of sources of unfreedoms : poverty, tyranny, poor eco-nomic opportunities, soeial deprivation, neglect of public facilities and repression by States.
According to Sen, the basic concern of human development is our capability to lead the kind of lives we have reason to value rather than the usual emphasis on increasing GDP per capita incomes.
Short Answer Questions
Question 1.
Explain the trends of Birth and death rates in India.
Answer:
The growth of population was checked by the high birth and high death rates in India before 1921. Birth rate during 1901 – 1921 fluctuated between 46 and 49 per thousand and the death rate between 44 and 49. So, ;the growth of population was little or negligible. After 1921. a clear fall ini death rae is noticeable. Death rate which was at 48.6 per thousand in 1911 – 20 came down to 7.2 per thousand in 2010 -11. But, the birth rate showed a slight decline initially and due to family planning drive birth rae also declined to 22.1 per thousand in 2010 = 11.
For the last sixty years, there is a steady fall in the infant mortality. In the second decade of the 20th century, infant mortality rate was 218 per 1,000 live births and it is 47 per 1,000 live births in 2010, Over the years, maternal mortality has also declined. It is 210 per 1 lakh births in 2007 – 2009.
Thus, the high growth rate of population can be explained in terms of high birth rate but a relatively fast declining death rate. Kerala, Tamil Nadu, Andhra Pradesh, West Bengal, Karnataka, Maharashtra and Punjab have achieved a birth rate below 20 per 1,000. These state are in the 3rd staghe of demographic transition. But, Haryana and Gujarat which occupied a high place in India in terms of per capita income far behind in reduction of birth rate. Uttar Pradesh, Rajasthan, Bihar and Madhya Pracjesh have a very high birht rate in the range of 25 – 31 per thousand.
These states are in the 2nd stage of demographic transition. It is not easy to bring down the birth rate, when the socio-economic conditions favour a larger family. Still, family planning has not become a way of life for many people. People’s attitudes towards marriage, family, family planning must change to achieve a substantial decline in the birth rate.
![]()
Question 2.
Explain the sex ratio in India.
Answer:
The sex ratio is defined as the number of females per 1,000 maks. Explains the sex ratio in IUndia. The sex ratio declined from 972 in 1901. to 946 in 1951 and to 927 in 1991, It is a disturbing featue. Subsequently there is a marginal improvement in the sex ratio. It is increased to 933 in 2001 and to 940 in 2011. Kerala alone shows a higher proportion of females of 1,084 per 1,000 males in 2011. in Punjab and Haryana, females account for 893 and 877 per 1,000 males in 2011 respectively which are at the bottom. Poverty, highte female infant mortality rates, hnigh mortality rates among women in reproductive ages and sociological factors are responsible for declining sex ratio.
Question 3.
Describe the family planning programme in India.
Answer:
Family Planning Programme
Importance of the family planning programme as a device to control population explosion is now universally recognised. Widespread use of contraceptives has contributed most to China’s success. About 85% of married women of child-bearing age use contraceptives in China a against 41% in India. The following aspects have to be discussed in this respect.
1. Public Information Programme :
For raising the level of consciousness, couples in the reproductive age are to be informed about the usefulness of family planning. The government is using all media to publicise the importance of family planning. Once they catch the idea of family planning, they themselves starty practising it.
2. Incentives and Disincentives :
The government has introduced different schemes in which incentives are given to those who accept family planning. Cash prizes have given some inducement to the people to go for sterilisation. In India family planning is voluntary. During the emergency, some excesses were committed and forcible sterilisations were done. In fact, atleast for some time, compulsory family planning is required.
3. Family Planning Centres :
Establishment of family planning centres is an integral part of family planning programme. These centers provide various clinical facilities needed for family planning. Contraceptive distribution centres are also playing very important role.
4. Research :
Research in the field of demography, communication action, reproductive biology and fertility control must be given priority. The government of India has realised this to obtain maximum results.
Question 4.
What is the relation between economic development and occupational distribution .
Answer:
Transfer of population from agriculture to industry and eventually to services is considered as an index of economic development. Colin Clark argues that “a high average level of real income per head is always associated with a high proportion of the working population engaged in tertiary industries, low real income per head is always associated with a low proportion of the working population engaged tertiary production and a high percentage in primary production”.
A.G.B. Fisher also said the same :
‘We may say that in every progressive economy there has been a steady shift of employment and investment from the essential primary activities to secondary activities of all kinds and to a still geater extent into tertiary production”. Simon Kuznets also observed the sae and says that when the development of a country takes place, the percentage of population engaged in primary sector shifts to industry and later to service sector. According to Hans Singer, economic development will be achieved by transforming a 85% agricultural dependent country in to just 15% agriculturally dependent country.
Occupational Distribution of Working Population in India :
Data provided in reveals that, over the period 1951 to 2010. agriculture remained the main occupation of the people. Over the period 1951 to 1971, the percentage of labour force engaged in primary sector remained unchanged at around 72%. There is a major change in the period 1991 – 2010 with the percentaghe of labour force in the primary sector falling to 51% in 2010 from 67% in 1991.
Question 5.
Explain the concept of Human resource development and its importance.
Answer:
Theodore W. Schutlz has argued that investment in education enhances human capital formation. It production is carried out without it and only with the help of unskilled and unedu- • cated labour, the production will fall catastrophically from its existing level.
Any activity which augments man’s productive capacity contributes to the human resource develoopment. Schultz listed the following five such activities :
- Health facilities and services, all expenditures which affect the life expectancy, strength and stamina, and the vigour and vitality of the people;
- On-job training including old style apprenticeships organised by firms;
- Formaly organised education at the elementary, secondary and higher levels;
- Study programmes for adults which are not organised by firms including extension programmes notably in agriculture; and
- Migration of individuals and families to adjust to changing job opportunities.
Amartya Sen also emphasizes the importance to be given to human resource development, where in he utilises entitlement and capability approach. Entitlements of individuals, especially women, can increase through education as it is considered as an asset and capability refers to one’s own wellbeings as healthy people can contribute a lot for the development of an economy. Here also health care systems where women’s health should be properly taken care, as they usually suffer from certain disabilities from childhood due to lack of proper nutrition and more usually suffer from certain disabilities from chilhood due to lack of proper nutrition and more attention should be bestowed on improving their capabilities for their active work participation.
Importance of Human Resource Development :
Education is moe important as it contributes most to the development of human resources.
Human resources development plays an important role in economic development. Effective use of physical capital itself is dependent upon human resources. Technical, professional and administrative people are required to make effective use of material resources. That is why, more investment in human resources is required, Countries are not developed due to underdevelopment of human resources. The general masses in these countries are either illiterate or with very low level of education, many are unskilled and untrained, and their general health is very poor. The development of human resources and the process of economic development both proceed together and reinforce one another.
Question 6.
Explain the National Health Policy, 2017.
Answer:
The National Health Policy, 2017 envisages providing larger package of assured compre-hensive primary health care through the health and wellness centres. The policy aims to attain the highest possible level of health and well – being for all through a preventive and promotive health care and universal access to quality health services without anyone having to face financial hardship, This would be achieved through increasing acess, improving quality and lowering the cost of health care delivery.
The highlights of the policy are (i) assurance based approach, (ii) micronutrient deficiency, (iii) Make-in-India initiative, and (iv) application of digital health. One of the mandates of the NHP, 2017 is the use of information technology towards health, care.
Key Targets of the National Health Policy, 2017, are as follows :
- Increase health expenditure of government from the existing 1.15 per cent to 2.5 per cent of the GDP by 2025.
- Increase life expectancy at birth from 67.5 years to 70 years by 2025.
- Reduction of total fertility rate (TFR) to 2.1 national and sub – national level by 2025.
- Reduce infant mortality rate (IMR) to 28 by 2019. In 2016 the IMR was 34 per 1000 live births.
- To redice the prevalence of blindness to 0.25% 1000 by 2025 and disease burden by one third from current levels.
- Incease utilization of public health facilities by 50% from current levels by 2025.
- More than 90% of the newborn are fully immunized by one year of age by 2025.
- Ensure skilled attendance at birth above 90% by 2025.
- Relative reduction in prevalence of current tobacco use by 15% 2020 and 30% by 2025.
- Access to safe water and sanitation to all by 2020 (Swachh Bharat Mission).
- Increase the share of stat on health to more than 80% of their budget by 2020.
![]()
Question 7.
Explain the method to construct Human Development Index.
Answer:
UNDP Human Development Report, 1997 describes human development as “the process of widening people’s choices and the leel of well-being they achieve. Regardless of the level of development, the three essential choices are to lead a long and healthy life, to acquire knowledge and to have access to the resources needed for a decent standard of living. Ohter choices highly valued by many people, range from political, economic and social freedom to opportunities for being creativbe and productive and enjoying self respect and guaranteed human rights”.
According to Mahbub-UI-Haw, “the difference between the economic growth and the human development schools is that the first exclusively focuses on the expansion of only one choice income – while the second embraces the enlargement of all human choices – whether economic, social, cultural of political”.
Construction of Human Development Indes (HDI) :
HDI measures the average achievement in three basic dimensions of human development and these are : (i) a long and healthy life as measured by life expectyancy at birth, (ii) knowledge as measured by the adult literacy rate and the gross enrolment ratio and (iii) a decent standard of living as measured by GDP per capita (PPP US$).
Before calculating HDI, an index for each of the three dimensions is created. For this, maximum and minimum values are chosen for each indicator as given below :
| Indicator | Maximum Value | Minimum Value |
| 1. Life Expectancy at Birth | 85 | 25 |
| 2(i). Adult Literacy Rate | 100 | 0 |
| (ii) Gross Enrolment Ratio | 100 | 0 |
| 3. GDP Per Capita (PPP US $) | 40,000 | 100 |
Performance in each dimension is expressed as a value between 0 and 1 by applying the formula given below :

The HDI is calculated as a simple average of the dimension indices.
According to HDR 2011, countries are grouped under four categories :
(1) countries in the HDI range 0.8 and above are in the very high human development group, (2) countries in HDI range 0.7 to 0.8 are in the high human development group, (3) countries in the HDI range 0.5 to 0.7 are in the range of medium human development group, and (4) countries in the HDI range less than 0.5 are in the low human development group.
India which was ranked at the 134th position in HDI in 1975 had improved its rank to 128 in 2005, but in 2011 its position slipped again to 134th rank. Norway ranked first and Australia ranked second in 2011.
India was at 135th position in HDI out of 187 countries in 2013. As per annual HDI – 2019. report, India ranked at the 129th position in 2018 out of 189 countries.
Question 8.
What do you mean by Gender Related Development Index (GRDI) and Human Poverty Index (HPI)?
Answer:
Gender Related Indices : Human Development Report, 1995 introduced two global gender indices. These are : (l) Gender related Development Index (GDI) and (2) Gender Empowerment Measure (GEM).
The GDI attempted to capture achievements throught the same set of basic capabilities as included in the HDI – life expectancy, educational attainment and income. HDI will be adjusted for gender inequality. The greater the gender inequality in basic human development, the lower GDI compared to HDI. The greater the difference between HDI and GDI, the more is the inequality. Near gender equality exists in Norway, Canada, United States, United Kingdom, Japan, Sri Lanka, China and Indonesia and gender inequality exists i Saudi Arabia, Pakistan, Iran, India and Nigeria. There is a greaer awareness in the world about gender inequality and efforts are being made to reduce gender inequality. Women movements are promoting and working for gender equality.
The Gender Empowerment Measure (GEM) indicates whether women are able to participate actively in economic and political life. It focuses on political participation (women’s share in parliament seats), economic participation (share in higher level and professional opositions) and power over economic resources (income gaps).
Human Poverty Index (HPI) :
Human Development Report, 1997 introduced the concept of Human Poverty Index. This index concentrates on deprivation in three essential elements of human life already reflected in HDI – longevity, knowledge and a decent living standard. HDR, 2009 used the following variables for calculating HPI : (i) percentage of people expected to die before age of 40 years, (ii) percentage of adult illiterates, (iii) percentage of people with access to health services and to safe drinking water and (iv) percentage of malnourished children under five years. Human Poverty Index for developingh countries reveals the existence of high value of HPI in Niger, Bangladesh, Pakistan and India.
Question 9.
Explain the concept of gross national happiness Index.
Answer:
Gross National Happiness Index : Countries like Bhutan are measuring their development with gross national happiness index. There is a need to bring a change in the existing method of measuring the development.
Gross National Happiness has been devised by Bhutan as an alternative indicatror for GDP to measure progress or development. The term Gross National Happiness (GNH) was coined by the Fourth king of Bhutan, Jighme Singye Wangchuck in the 1970’s. The concept implies that sustainable development should take a holistic approach towards notions of progress and give equal importance to non – economic aspects of wellbeing. The GNH index is constructed based upon a multidimensional methodology known as the Alkire – Foster method.
The concept of GNH is explained by four pillars :
Good governance, sustainable socio – economic development, cultural preservation and enviromental conservation. These four pillars are further classified into nine domains : Psychological wellbeing, health, education, time use, cultural diversity and resilience, good governance, community vitality, ecological diversity and resilience, and living standards. All domains are weithted equally. The domains represent 33 indicators (variables) of Wellbeing. The weights of the various variables in a domain are unequal. In general, subjective indicartors have been given lower weights than objective indi-cators.
In happiness, averages do not count and that is why, within each indicastor, a ‘sufficiency target’ is set. A person is considered ‘happy’ under this indicator when the ‘sufficiency’ level is achieved. Based on answers for the 33 indicators, judgement is given how a person is happy in the following way.
Sufficiency in 77% – 100% of the indicators : deeply happy.
Sufficiency in 66% – 76% of the indicators : extensively happy.
Sufficiency in 50% – 65% of the indicators : narrowly happy.
Sufficiency in 0% – 49% of the indicators : unhappy or not – yet – happy.
Very Short Answer Questions
Question 1.
Birth rate.
Answer:
It is the Ratio of number of births per 1,000 population in a year. Birth rate during 1901 – 1921 fluctuated between 46 to 49 per 1,000 population. Birth rate declined to 21.8 per 1,000 in the year 2010 – 11.
Question 2.
Death rate.
Answer:
It is the Ratio of deaths per 1,000 population in a year. The death rate during 1901 -1921 fluctuated between 44 and 49 per 1,000 population. It was 48.6 per 1,000 population in 1911 – 20. It was reduced to 7.1 per 1,000 in 2010 – 11.
![]()
Question 3.
Infant mortality rate.
Answer:
It is the ratio of number of deaths per 1,000 bom children in a year. In the second decade of the 20th century, this rate was 218 per 1,000 live birth and it is 47 per 1,000 live births in 2010.
Question 4.
Maternal Mortality Rate.
Answer:
‘It is the ratio of numer of delivery deaths for, lakh women in a year, over the years maternal mortality rate has also declined. It was 210 per 1 lakh live births in 2007 – 09.
Question 5.
Sex ratio.
Answer:
It is the number of females per 1,000 males. This ratio was declined from 972 in 1901 to 946 in 1951 and 927 in 1991. It is increaed to 933 in 2001 and 940 in 201. Poverty, higher female infant mortality rates, high mortality rates among Women in reproductive ages are responsible for declining sex ratio.
Question 6.
Population explosion.
Answer:
Population increases faster than food supply and this imbalance leads to over population and this is called “population explosion”.
In the second stage’ of the theory of demographic transition, due to substantial reduction in the mortality rate and no corresponding decline in the birth rate, rapid growth of population exists. In this stage population increases at an alarming rae and economists called it “population explosion”. India had faced this problem during the period 1951 – 1991.
Question 7.
Contraceptives.
Answer:
Contraceptives are one of the family planning method to control population. The family planning centres provide contraceptive distribution centres.
Question 8.
Literacy rate.
Answer:
The reading and writing skills of a person is known as literacy. The literacy rate Can be studied with the help of following formula.

The literacy rate is improved form 18 percent in 1951 to 74 percent in 2011. similarly male leteracy improved from 27 percent to 82 percent and female literacy from a percent to 66 percent in the same period.
Question 9.
National Rural Health Mission.
Answer:
This scheme was introducedd during 11th plan. It intends to increases access and utilisation of quality health by stregthening health infrastructure. It was planned to have accredited social Health activistis (ASHA’s) by 2008. All sub centres functional with 2 auxilliary nurse midwines (ANMs) by 2010. mobile medical unit for each district by 2009.
![]()
Question 10.
Janani Suraksha Yojana.
Answer:
Janani Suraksha Yojana :
This programme was started in the year 2005. This scheme is meant for promoting health and nutrition to women and child. It has 2 objectives.
- Reducing Infant Mortality Rate
- Reducing Maternal Mortality Rate.
It is a gradual approach of increasing istitutional capacity encouraging institutional deliveries will ensure success of the scheme.
Question 11.
National Urban Health Mission.
Answer:
It is intended to meet health needs of uraban poor, particularly the slum dwellers and other marginalized dwellers who may be in slums or citites. This programme covers all cities with a population of 1 lakh and above.
Question 12.
Gender empowerment measure.
Answer:
This focuses on women’s participation in economc and political life and their power over econonmic resources. This concept also indicates whatever the women’s share in parliament seats, share in higher level and professional positions, and income gaps.
![]()
Question 13.
HumcCn poverty Index (HPl)
Answer:
The concept was introduced by the human development report 1997. This index concentrates on deprivation in three essential elements of human life already reflected in HDI that is longivity, knowledge, and a decent living standard. HDR 2009, used the following variables for calculating HPI, percentage of people expected to die before age of 40 years, percentage of adult illeterates, percentage of people with access to health services and to safe drinking water.